Interpretation of results
NOTE! To get an overall picture and to make an accurate diagnosis KMScreen test should be seen as one of several tests that measures eye abnormalities.
In order to interpret the survey results, you must have the following four questions in mind:
1. What type of strabismus, has the patient?
Is it a vertical strabismus, horizontal, or a combination strabismus in which there is both vertical and horizontal strabismus?
2. Is the squint paralytic or non-paralytic, and is there a mechanical obstruction in one or both eyes?
3. Is there A or V phenomenon?
4. Is there torsion (tilt)?
1. What type of strabismus, has the patient?
Is it a vertical strabismus, horizontal, or a combination in which there is both vertical and horizontal strabismus?
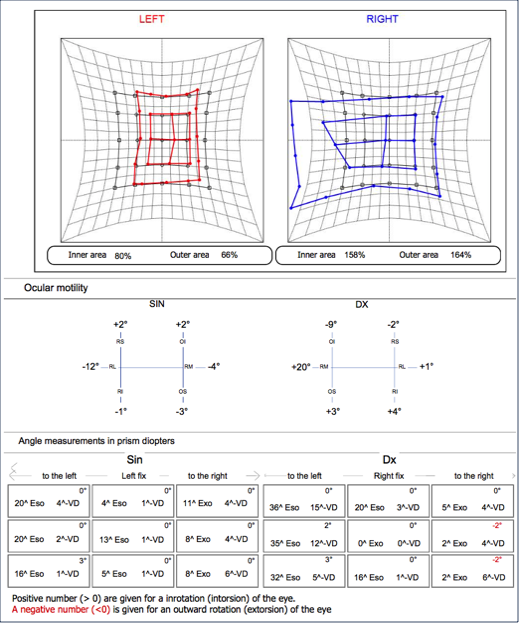
The answer to patient example: In the primary position we see tthe most displacement of the eyes are in the vertical position. And because of the two flags position we can see that we have a left over right hypertropia. We will now focus on the vertical muscles
2. Is the squint paralytic or non-paralytic, and is there a mechanical obstruction in one or both eyes?
Here we can clearly see that we have a paralytic strabismus
The right eye flag is significantly smaller than the left eye flag. This is confirmed by the computer's calculation of the two-eyes outer area calculation. The Right eye's outer area is 60% of the normal eye (100%) gaze range.
What we have found so far is that it is a paralytic vertical strabismus where the smallest flag (that is, the paralytic eye) is the right eye.
We continue to focus on the right eye's vertical muscles to see if we can find one or more muscles with the strongest paralytic restriction.
We are now looking at the left eye's ocular motility chart, and we see directly that the superior rectus muscle has a 21 degree underfunktion (-21°). This leads us directly to the diagnosis that we have an right sided oculomoturius nerve paresis
Left eye fix
Right eye fix
Left eye fix
Right eye fix
Exampel: Step by step interpretation of the result
1. What type of strabismus, has the patient?
Is it a vertical strabismus, horizontal, or a combination in which there is both vertical and horizontal strabismus?
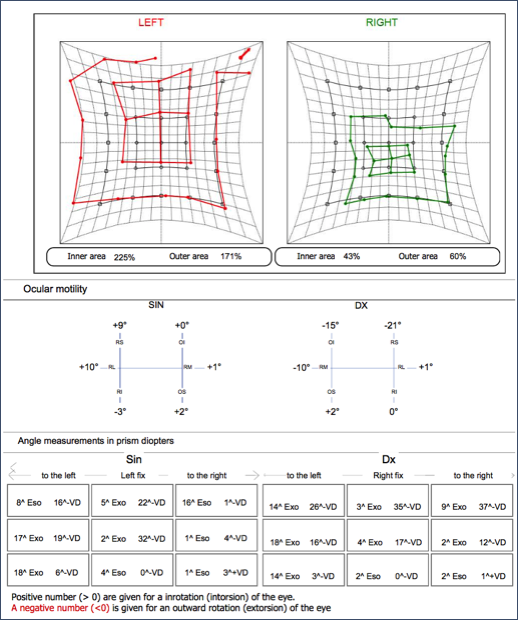
The answer to patient example: In the primary position we see tthe most displacement of the eyes are in the horisontal position. And because of the two flags position we can see that we have an eso(tropia). We will now focus on the horisontal muscles
2. Is the squint paralytic or non-paralytic, and is there a mechanical obstruction in one or both eyes?
Here we can clearly see that we have a paralytic strabismus
The left eye flag is significantly smaller than the right eye flag. This is confirmed by the computer's calculation of the two-eyes outer area calculation. The left eye's outer area is 66% of the normal eye (100%) gaze range.
What we have found so far is, that it is a paralytic horisontal strabismus where the smallest flag (that is, the paralytic eye) is the left eye.
We continue to focus on the left eye's horisontal muscle to see if we can find one muscle with the strongest paralytic restriction.
We are now looking at the left eye's ocular motility chart, and we can see directly that the lateralis rectus muscle has a 12 degree underfunktion (-12°). This leads us directly to the diagnosis that we have an left sided abducens nerve paresis (in this patient case, the pasient has a iatrogen-abducens pares
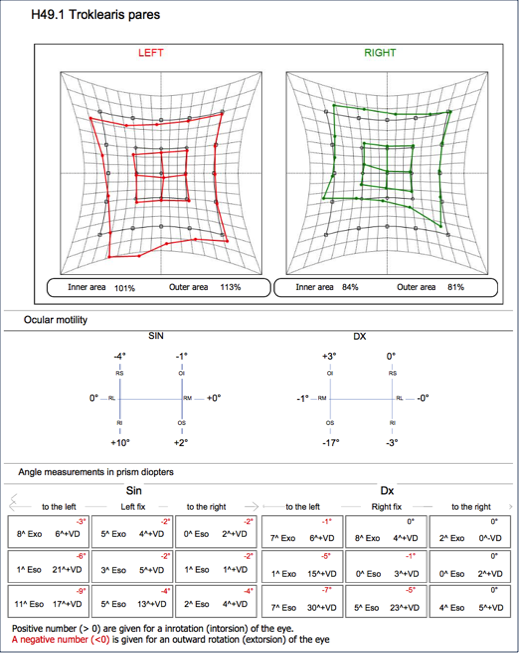
1. What type of strabismus, has the patient?
Is it a vertical strabismus, horizontal, or a combination in which there is both vertical and horizontal strabismus?
The answer to patient example: In the primary position we see tthe most displacement of the eyes are in the vertical position. And because of the two flags position we can see that we have a right over lrft hypertropia. We will now focus on the vertical muscles
2. Is the squint paralytic or non-paralytic, and is there a mechanical obstruction in one or both eyes?
Here we can clearly see that we have a paralytic strabismus
The right eye flag is significantly smaller than the left eye flag. This is confirmed by the computer's calculation of the two-eyes outer area calculation. The right eye's outer area is 81% of the normal eye (100%) gaze range.
What we have found so far is that it is a paralytic vertical strabismus where the smallest flag (that is, the paralytic eye) is the right eye.
We continue to focus on the right eye's vertical muscles to see if we can find one or more muscles with the strongest paralytic restriction.
We are now looking at the right eye's ocular motility chart, and we see directly that the superior obliquee muscle has a 17 degree underfunktion (-17°). This leads us directly to the diagnosis that we have an right sided trochlear nerve pares
4. Is there torsion (tilt)?
When we have the most underfunction in the vertical muscles we will always examine the torsion of the eye's position.
In this patient case, we see that the highest torsion is in the direction of the right eye Superior Obliquee, -9 degrees extorsion with the right eye fixation and -7 degrees extorsion of the eye when the left eye fixate. This confirms our diagnosis.
Right Superior Obliquee palsy